
Executive Summary
The Food Standards Agency (FSA) is the UK government department responsible for protecting public health with regards to food safety. Campylobacter is the leading bacterial cause of foodborne illness in the UK. Cases are most frequently attributed to chicken, so in 2010, the FSA began a Campylobacter reduction programme to reduce Campylobacter contamination levels in poultry. Working with industry, the FSA was able to successfully reduce the proportion of chickens highly contaminated with Campylobacter (> 1,000 cfu/g) at retail from 19% in 2014 to 5% in 2017; recent data indicates these levels have been maintained. Unfortunately, human cases have remained stable at around 100 per 100,000 population.
An expert elicitation exercise was run to generate testable hypotheses that might explain why the reduction in highly contaminated chicken carcasses available at retail did not correspond to decreased levels of human disease. Experts were recruited with a variety of experience in either poultry production or Campylobacter research. The experts individually generated 157 hypotheses; condensing together similar ideas resulted in 25 final hypotheses. The second round of the exercise involved the experts ranking these hypotheses against the criteria “What are the most likely explanations for campylobacteriosis case numbers not following the trends seen with Campylobacter levels in chickens at retail?” This resulted in eight hypotheses being ranked most likely to explain the Campylobacter situation in the UK and also provided information on the availability of evidence to investigate these hypotheses. The top hypothesis when focussing only on the ranking from the experts on the above question was related to 1,000 cfu/g being the wrong target to focus on. When considering the available evidence alongside the ranking, the hypothesis concerning imported poultry meat came out on top.
This exercise is part of a larger programme of work by the FSA to review its previous Campylobacter reduction efforts and explore new strategies to reduce Campylobacter infections in humans. The results of the expert elicitation will be used to inform the FSA’s work in these areas.
1. Introduction
Since 2005, Campylobacter infections have been the most commonly reported zoonosis in EU member states (EFSA, 2023). Source attribution studies in the UK and other EU countries have identified chickens and chicken meat as the most frequent cause of Campylobacter infections (Brinch et al., 2023; Cody et al., 2019; Domingues et al., 2012; McCarthy et al., 2021). An EU baseline survey in 2008 identified that in the UK, 27.1% of samples from broiler carcasses were highly contaminated (meaning they contained more than 1,000 bacterial colony-forming units (CFU) per gram of neck skin removed from whole processed chickens) (EFSA, 2010). To address this, the FSA began working with the poultry industry in 2010 to reduce the levels of Campylobacter spp. contamination in raw chicken meat from broilers. A target was set to reduce the prevalence of the most contaminated broilers to below 10% at the end of the slaughter process, which was estimated to equate to 7% at retail, by 2015 (FSA, 2010, 2015).
FSA studies performed on chicken at retail demonstrated that between 2014 and 2017, the proportion of chickens at retail with greater than 1000 cfu/g dropped from 19% to 5% (FSA, 2020); levels of highly contaminated carcases have remained stable since then (data held by FSA from retailers). When setting the original target, modelling suggested that introducing interventions at the farm and slaughterhouse level could lead to a 15-30% reduction in human cases (FSA, 2010). However, cases of campylobacteriosis recorded in national surveillance in the UK have remained steady at around 100 cases per 100,000 population between 2014 and 2019 (UKHSA, 2024).
The Advisory Committee on the Microbiological Safety of Food (ACMSF), the Scientific Advisory Committee that provides independent advice to the FSA, has produced several reports on Campylobacter; their last report, published in 2019, was initiated because of the “continued dominance of Campylobacter as the leading bacterial cause of foodborne disease in the UK” (ACMSF, 2019). Following this, the FSA is reviewing its Campylobacter reduction campaign to understand why the reduction in Campylobacter prevalence in chicken meat was not associated with a decrease in human cases. The reasons for this discrepancy between retail levels and human cases are likely complex and multifactorial. An expert elicitation exercise was run to generate hypotheses for likely reasons and these were then prioritised in order of likelihood. These results will help determine areas on which the FSA can focus its Campylobacter efforts.
2. Methods
The Delphi technique, using two rounds of participation, was used to gather and prioritise responses from the experts (Avella, 2016). Experts were identified based on previous Campylobacter-related contributions to the FSA’s work or from recent publications in the scientific literature. Individuals were invited by email and asked to consent to participate by responding to the invitation. A snowballing recruitment approach was used, so that participants were asked to recommend additional contacts to increase the pool of experts. Members of the UK’s ACMSF were also invited to participate. Other than the ACMSF participants, experts were not aware of the identity of other participants.
All participants were provided with an information pack (see Supplement 1) providing information on campylobacteriosis cases in the UK, levels of Campylobacter measured in chickens at retail, and highlighting previous work on Campylobacter performed by the FSA. In the first round of the exercise, participants generated hypotheses for the question “Why do you think that the reported Campylobacter cases in humans have not gone down when we’ve successfully reduced levels in chicken at retail?” and were invited to submit evidence to support these hypotheses or research project suggestions to test them. Participants were allowed to suggest up to 10 hypotheses. They were also invited to answer questions related to their sector of work, area of expertise, and rank their knowledge of Campylobacter. The first round of the expert elicitation was completed using Microsoft Forms.
The second round of the exercise was completed in Microsoft Excel and results were analysed in Excel and R statistical software (v4.3.2; R Core Team, 2023). Participants were asked to choose the top five hypotheses capable of explaining the steady rate of UK campylobacteriosis cases from the condensed list of possible explanations generated after the first round of the exercise. They were also invited to weight how important or likely the hypotheses were in explaining Campylobacter steady case rates, with the weights adding up to 100%. A few experts declined to provide a weighting; in these situations, the researchers applied an even weighting across the suggested hypotheses.
For the prioritisation, the ranking and the weighting were considered. Ranking was determined by adding up the number of times all experts chose a hypothesis for each question. The weighting for each hypothesis was calculated by adding up the total weighting for that hypothesis and dividing by the total sum of all weights from all hypotheses for that question.
3. Results
3.1. Details of experts
Ahead of the exercise, 41 experts agreed to participate and were sent the information pack. Participants were recruited from the UK, Ireland, Denmark, the Netherlands and France. During the first round of the exercise, experts were asked to provide details on the sector of their work, which area of chicken production or Campylobacter research they were most familiar with, and how they categorised their knowledge of Campylobacter. Responses from the 35 experts that completed the first round of the exercise are given in Tables 1-3 below; six experts did not respond. This information was collected for background purposes only and was not included in further analysis; the decision to include all participants equally despite their familiarity with Campylobacter was because only one participant gave a familiarity score below a “3” (Table 3). More experts from academia, followed by government, were represented compared to industry participants. Experts were only allowed to select from one area of expertise, where “microbiology” was represented much more strongly than other areas.
3.2. First round: hypothesis generation
In the first round of the expert elicitation, participants were asked to come up with hypotheses explaining:
- Why do you think that the reported Campylobacter cases in humans have not gone down when we’ve successfully reduced levels in chicken at retail?
Along with the generated hypotheses, they were also given the option to answer:
-
What evidence is available that supports your hypothesis?
-
What research projects would be necessary to explore the hypothesis?
The experts generated 157 individual hypotheses; for those hypotheses, the “available evidence” field was completed 133 times and the “research projects” field 128 times. The full list of hypotheses, available evidence, and suggested research projects provided by the experts can be found in Supplement 2 (“Rd1 all hypos” sheet).
All hypotheses were reviewed by the authors (EK, IF, JJ, WP) to identify common themes and categories from the available hypotheses. These groupings were reviewed until the research team felt all ideas contained within the individual hypotheses were reflected in the grouped hypotheses, leaving 25 explanations (Table 4; full descriptions of the hypotheses can be found in Supplement 2 “Rd2 results”); some of the hypotheses (for example, “improving qualitative demographic data of campylobacteriosis cases”) were considered to be evidence or project suggestions and were not captured in the condensed hypotheses. The assignment of the grouped hypotheses to the individual hypotheses can be found in Supplement 2 (“Rd1 recoded” sheet).
Table 4 shows the number of times the hypotheses were suggested in the first round; some hypotheses spanned multiple consolidated hypotheses, so the number of reported hypotheses in Table 4 is greater than the 157 reported above. Many of the condensed hypotheses could be further grouped into categories; these categories are included in Table 4 and the number of times they correspond to a condensed hypothesis is provided in Table 5.
3.3. Second round: ranking and weighting of hypotheses
To prioritise the generated hypotheses, the experts ranked and weighted the hypotheses in the second round of the exercise, considering the following questions:
-
Question 1: Which hypotheses do you think are the most likely reason Campylobacter cases have not dropped in humans?
-
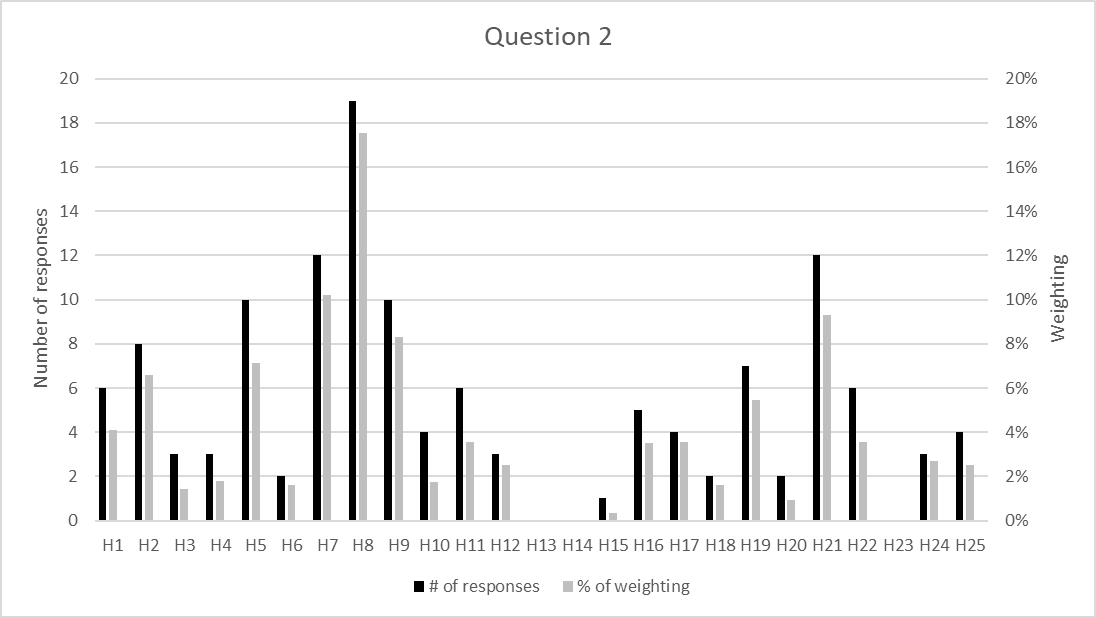
Question 2: Which hypotheses likely have the most data currently available to investigate?
-
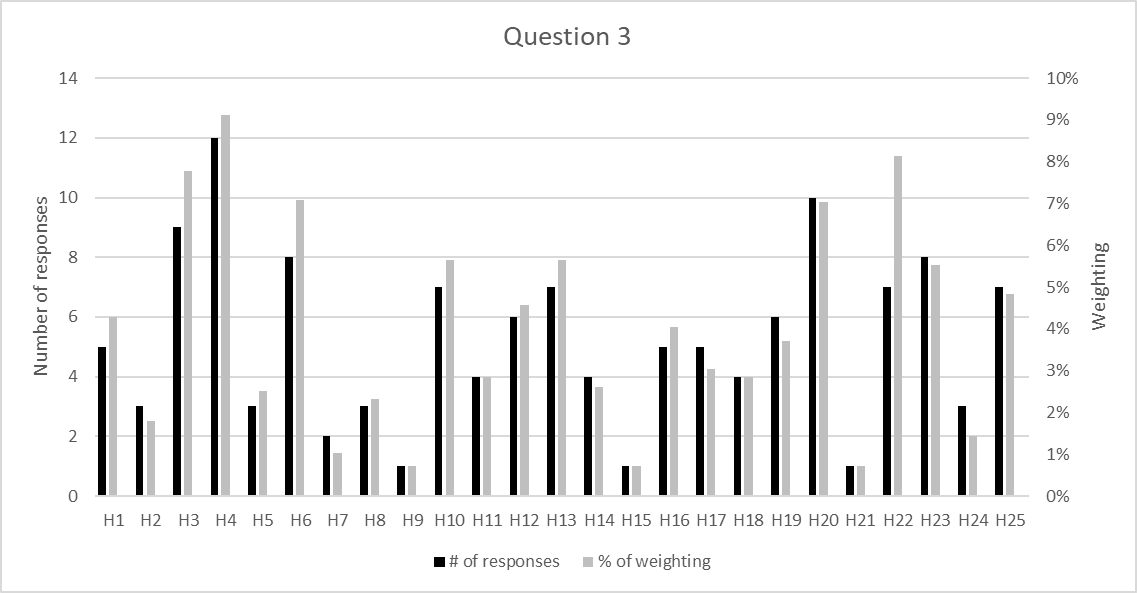
Question 3: Which hypotheses have the most uncertainty related to them?
Figures 1, Figure 2 and Figure 3 show the results for each question. Full results of the second round of the exercise can be found in Supplement 2 (“Rd2 results” sheet). For each question, the number of responses correlated strongly with the weighting (Q1; r = 0.946, Q2; r = 0.986, Q3; r = 0.954). For Question 2 and Question 3, the responses negatively correlated by both number of responses (r = -0.51) and the weighting (r = -0.48), suggesting that when experts felt there was more data available for a particular hypothesis, the uncertainty associated with it would drop.



3.4. Prioritisation of the hypotheses
Ranking of the hypotheses was done based on the weighting since this encompassed the expert’s confidence that the response addressed the question. To simplify the weightings for each question, they were split into groups based on tertiles in the data. For question one and two, this created groups where High = ≥5% weighting; Medium = 3-4% weighting; Low = ≤2% weighting. For question three, the groups created corresponded to High = ≥6% weighting; Medium = 4-5% weighting; Low = ≤3% weighting.
In the first instance, the hypotheses were ranked based on their weighting for Question 1 to identify those considered most likely to explain why human campylobacteriosis levels in the UK do not reflect the reduction achieved in the highest levels of contamination in chickens at retail. Table 6 shows the top eight hypotheses ranked as “high” for Question 1; within these eight, the results have also been ranked by weighting for Question 2 in the first instance and then Question 3. The rankings of all hypotheses by question can be found in Supplement 2 (“Rd2 sorted” sheets).
3.5. Comparison of results between rounds
Of the eight hypotheses that were ranked most likely to explain why Campylobacter cases have not dropped in humans in round two of the exercise, six of them were also suggested most often in the first round (Table 7). Hypothesis “H24: inadequate controls during slaughter and processing” ranked highly in round 2 (tied at 6% weighting with “H8: imported poultry meat”, “H17: sampling wrong products/areas/times” and “H19: other sources- food”) but came in about a third of the way down in the number of times that hypotheses were recommended in round 1 (suggested 8 times). Similarly, hypothesis “H21: changing diagnostic methods” was ranked “high” for round 2’s question 1, but came in 9th place in round 1, having been suggested 7 times.
4. Discussion
This expert elicitation exercise has generated and prioritised hypotheses to help explain the current Campylobacter situation in the UK, where overall human campylobacteriosis cases have remained fairly steady despite the FSA’s and industry’s work to reduce the levels of chickens available at retail which are highly contaminated with Campylobacter. The ranked hypotheses will be considered by FSA scientists and policy colleagues to help focus the FSA’s research into this issue. This will be further aided by the evidence and research suggestions provided by the experts in the first round of the exercise. This is to support continued efforts by the FSA to reduce the number of foodborne cases of Campylobacter by revisiting its Campylobacter Reduction Programme.
Prioritisation of the FSA’s work based on this expert elicitation exercise will be guided by the weighting for question 1 of round 2 (“Which hypotheses do you think are the most likely reason Campylobacter cases have not dropped in humans?”). Within the eight hypotheses ranking “high” (>= 5% weighting), feasibility of addressing the hypotheses will be guided by the weightings of question 2 (current data availability) and question 3 (uncertainty), with priority given to those with data already available or low uncertainty. As decisions are made on exploring hypotheses, the FSA will move further down the list from question 1 rankings to start investigating medium then low ranked hypotheses. Alternatively, hypotheses ranked “high” for question 2, those with easily available evidence, could be explored for quick determinations of their contribution to campylobacteriosis cases in the UK.
As the campylobacteriosis case trends analysis demonstrated (see Supplement 1, Figures 8 & 9), the UK is not the only country to see case numbers remain steady, or even increase, despite public health efforts and industry intervention strategies to reduce them. During our elicitation exercise this was noted by the experts, with comments during the first round including “similar trends in a lack of reduction in cases of Campylobacteriosis and retail meat have been noted elsewhere” and “[you have identified] an international issue, more countries see the same thing”. Given the widespread nature of this issue, one of the experts noted after the second round of the exercise “some of the risk factors [proposed] do not explain why the pattern of no reduced cases can be observed all over the EU. We are probably looking at an effect that is not specific to UK”.
There were 5 “other sources” hypotheses that suggest that Campylobacter cases may not be restricted to exposure to strains from UK broiler production. Two of them (“H19: other food” and “H8: imported poultry meat”) were in the top 8 ranked hypotheses. This indicates the FSA may need to reconsider its focus when commissioning future work to have the best chance of making a significant reduction in campylobacteriosis cases in the UK. After poultry, ruminants have been associated with C. jejuni human infections and pigs with C. coli human infections (Cody et al., 2019; McCarthy et al., 2021).
4.1. Lessons learnt from the exercise
This exercise was run without a consensus meeting as the necessary amount of information could be obtained just from running the two response rounds. This allowed participants from a wide range of organisations to be invited since there would not be difficulty in trying to schedule a consensus meeting. Some participants noted that they would have appreciated a consensus meeting to further discuss the hypotheses and alter their second-round rankings based on these discussions. While the objectives of the exercise (prioritising hypotheses for why UK campylobacteriosis cases have not reduced in line with levels of high contamination at retail) were achieved, further refinement of these rankings would have been possible had a consensus meeting been held.
Several of the participants noted that some hypotheses were very similar (for example, “H16: sampling is not accurate” and “H18: stressed cells difficult to detect”) so they only chose one to include in the ranking. This means some of the scoring between two similar hypotheses might be split and not rank as highly as they otherwise would have been. Adding a step where the experts reviewed the choice of the consolidated hypotheses, either virtually or through a discussion meeting, would have helped prevent this issue. However, this option was not explored as it would have increased the amount of time the experts needed to spend on the exercise to review all the hypotheses and come to a consensus on a list of hypotheses that captured all ideas from the first round.
While most of the participants found the overall exercise relatively easy to complete, there were some issues with question 2 and 3 from the second round. For question 2, while it specifically asked about data “currently available”, one participant noted that some data might not be currently available but would be easily obtainable, which could assist in its prioritisation. If this exercise were repeated, two questions covering availability and ease of generation could be included. Many of the participants expressed confusion over how to interpret question 3, which had been left intentionally vague for the expert to interpret as they wished. Participants were not sure whether it was uncertainty over whether the hypothesis might explain the campylobacteriosis case trends or if there was uncertainty in the data that would be associated with the hypothesis. Some experts clarified their interpretation in their response, but most did not. It would have been beneficial to have provided more guidance to the experts on answering this question to make better use of the results for question 3.
4.2. Comparison of results to other works on Campylobacter
As noted previously, campylobacteriosis case rates in humans remain high across the EU. Several international organisations have reviewed what could be done to reduce levels of Campylobacter in poultry and reduce campylobacteriosis case numbers, focussing on interventions throughout the broiler production chain (Koutsoumanis et al., 2020; WHO, 2024). Both reports recognise that combining interventions is likely necessary in order to significantly impact Campylobacter levels and prevalence in poultry meat.
Similar reviews have been performed in the UK (ACMSF, 2019; Goddard et al., 2022). In 2019, the Advisory Committee for the Microbiological Safety of Food (ACMSF) published their third report on the management of Campylobacter. This extensive report generated many recommendations for the FSA to consider in evolving its strategy for reducing the incidence and risk of foodborne Campylobacter infection in humans. Sixteen of the hypotheses identified in this expert elicitation exercise were also encompassed in the recommendations that featured in the ACMSF report (Table 4). For example, our hypotheses “H1: More vulnerable consumers” & “H2: Changes in socioeconomic factors” were also recognised by the ACMSF as they recommended that the FSA continues to monitor socio-demographic differences in kitchen practices and experience of foodborne illnesses.
In the ACMSF report’s chapter on “Risks in the food chain: poultry”, the Committee concluded “no single practical intervention has been shown to be capable of eliminating Campylobacter”, then expanded that a combination of controls at the farm and processing levels could reduce levels (ACMSF, 2019). In 2022, Goddard et al. published a summary of evidence relevant to the Campylobacter situation in the UK, where they reached similar conclusions that a “multiple-hurdle” approach would be necessary to reduce campylobacteriosis cases in humans (Goddard et al., 2022). They recommended several research ideas to determine where interventions along various food production chains would have the biggest impact, including more detailed studies of intervention strategies, increased use of whole genome sequencing to better understand source attribution and transmission, and considering behavioural science and how consumers view their risk of becoming infected with Campylobacter (Goddard et al., 2022). The recommendations from both these reports, combined with the prioritised hypotheses from this expert elicitation exercise, will guide the FSA’s future work to reduce human case numbers caused by Campylobacter.
Acknowledgements
We would like to thank all the experts that provided their time and expertise to participate in this exercise (see Supplement #3). Additionally, we’d like to thank Darren Holland and Greg Wasinski at the FSA for their input during the development of this work.