
As part of the FSA’s responsibility for ensuring that food is safe we occasionally assess scenarios such as this one where a hazard does not yet occur in the UK, to ensure that we are better prepared in the event of an introduction.
Executive Summary
Since the first confirmed case on 25th March 2024, Highly Pathogenic Avian Influenza A (H5N1) clade 2.3.4.4b genotype B3.13 has been detected in dairy cattle across the United States. There is no evidence to suggest this virus is currently present in the UK or other European countries and it has not been detected in UK cattle. This assessment sets out the hypothetical risk to UK consumer health from consuming portions of beef and beef offal from infected herds, if the virus began circulating in UK cattle. The scope of this risk assessment includes thoroughly cooked, less than thoroughly cooked and raw, beef, minced beef and beef offal.
There is very limited evidence of transmission of avian influenza via food. Two US studies of cattle infected with H5N1 found viral RNA in a small proportion of postmortem muscle and kidney samples (0.5-1%). H5N1 influenza A virus was not detected in several different types of muscle tissues that correspond to common retail cuts of meat tested from one of these animals. In beef offal, H5N1 has been detected in lung samples at a titre of 2.8 Log10TCID50/mL and mammary glands at 7.3-7.810 Log TCID50/mL.
Cooking beef burgers at temperatures of over 63°C after artificially inoculating them with high levels of virus has been shown to reduce the level of H5N1 by 5.6 Log. We therefore assess that the probability of individuals being exposed to infectious doses of virus via a portion of thoroughly cooked beef, minced beef and beef offal to be Negligible, with Low uncertainty.
UK consumers may choose to consume beef and beef products that are less than thoroughly cooked. Evidence suggests that temperatures equivalent to those that result in “rare” meat (49°C) are effective at reducing the level of virus in food by 2.5 Log. Therefore, the probability that UK consumers will receive infectious exposures via a portion of less than thoroughly cooked beef, minced beef and offal is also considered to be Negligible. The uncertainty in this estimate is Medium, due to the lack of evidence on the distribution and titre of the virus in beef muscle and offal and the variations in processes and temperatures used to produce less than thoroughly cooked foods.
Consumers may also choose to eat raw beef, such as steak tartare and beef carpaccio. These products undergo no further processing that would reduce the infectivity of the virus if present. Therefore, the probability that UK consumers will receive infectious exposures via a portion of raw beef products such as carpaccio and beef tartare is considered to be Very Low. The uncertainty in this estimate is Medium, due to the lack of evidence on the distribution and titre of the virus in beef muscle.
In the event of infection, the severity of detriment has been determined as Low due to the mild presentation observed in cases so far in farm workers. However, this is with a Medium level of uncertainty as these cases are not believed to have been acquired via foodborne exposure and it is unknown whether severity of illness will be different compared to other routes of exposure such as inhalation.
Statement of purpose
The purpose of this assessment is to understand the risk to consumers from beef and beef products, including:
A. thoroughly cooked beef and minced beef
B. less than thoroughly cooked beef and minced beef
C. raw beef
D. thoroughly cooked offal
from UK beef and dairy cattle in the hypothetical scenario of an outbreak of HPAI H5N1 strain B3.13 in cattle in the UK.
Risk question
What is the per portion risk to UK consumers from meat, mince and offal from beef, in the hypothetical scenario that HPAI H5N1 strain B3.13 is found in UK beef and dairy cattle?
Hazard identification
The hazard considered for this assessment is an influenza A virus of avian origin classified as B3.13. Influenza viruses are negative-sense, single-stranded, enveloped RNA viruses classified in the family Orthomyxoviridae, and 80-120nm in diameter. Analysis of available sequences supports the hypothesis of a single bird-cow crossover event followed by cow-cow spread (ASTHO, 2024).
To date, there is no evidence to suggest Avian influenza A (H5N1) clade 2.3.4.4b genotype B3.13 is currently present in the UK or Europe (HAIRS, 2024).
Starting in January 2024, a number of dairy herds in the US were reported as exhibiting clinical signs including inappetence and milk drop. 10-15% of animals on affected farms showed clinical signs, with minimal deaths. At sites in Texas, deaths of wild birds (pigeons, blackbirds, and grackles) and domestic cats, assumed to have consumed unpasteurised milk, were also reported.
Although regional diagnostic labs were initially unable to identify a cause, samples received at the Iowa State University Diagnostic Laboratory in Ames on 24 March 2024 (Texas) and 25 March 2024 (Kansas) were found to be positive for influenza A virus (IAV) by PCR. A press release was issued on 25 March 2024 (APHIS, 2024) and an early-access manuscript fully describing these results was published on 29 April 2024 (Burrough, et al., 2024). Sequence analysis suggested the virus first infected cattle in November 2023 (Science.org, 2024).
On 25 April 2024, the FDA reported that PCR testing on samples from a nationally representative commercial milk sampling study found influenza virus RNA in around 20% of retail samples tested, although the number of samples tested was not given (FDA, 2024). On 26 April 2024 the FDA reported some preliminary results suggesting that pasteurisation is effective at eliminating infectious HPAI from milk (FDA, 2024).
Since its detection the outbreak has continued to spread. Several routes have been proposed as possible mechanisms for spread between farms and to other states. These include the movement of infected animals, the movement of contaminated milking equipment, and spread via wild birds (Burrough, et al., 2024).
There is a concern that the new strain could be introduced to livestock in the UK by migratory birds. The H5N1 reassortment virus implicated in the USA dairy cattle outbreak has never been detected in the UK or Europe. In addition to this, no other Eurasian-North American reassortment have been recorded in the UK or Europe, despite detections of these in North America since 2014. In Great Britain (GB), outbreaks of avian influenza on poultry premises are followed-up with sequencing and a proportion of wild bird cases are sequenced annually. No results to date suggest that this strain is present (HAIRS, 2024). This risk assessment is hypothetical and is based on a scenario that Avian influenza A(H5N1) clade 2.3.4.4b genotype B3.13 has entered the UK food chain.
Exposure assessment
Risk Pathway (UK Beef)
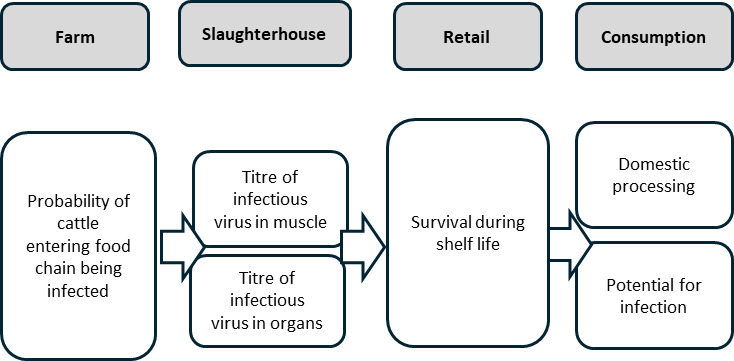
Farm: probability beef cattle being infected with B3.13
In May 2024 APHIS carried out a study of 109 beef muscle samples from condemned dairy cattle. No viral RNA was detected in 108 samples. Viral RNA was detected in tissue samples, including diaphragm muscle, from one cow (APHIS, 2024). We have no information as to the viability or titre of the virus in that positive sample (uncertainty). In September 2024, FSIS added testing for H5N1 influenza A in muscle samples from culled dairy cows to the national surveillance programs for pathogens and chemical contaminants. As of January 1, 2025, FSIS has results from 208 diaphragm muscle samples. Of these, samples from one dairy cow, as well the kidney from that animal, indicated a positive for H5N1 influenza A at very low levels. Additional sampling from that carcase, including several different types of muscle tissues that correspond to common retail cuts of meat, did not detect H5N1 influenza A virus (APHIS, 2024). There is currently no evidence of the clinical signs in non-lactating cattle (uncertainty).
Beef: titre of virus in beef (fresh meat, minced and offal) from infected cattle
Although limited information is available for influenza virus in cattle, we know that in infected birds the tissue distribution of influenza virus varies by strain and species. However, the proportion of cattle infections in which muscle tissue contains virus appears to be low. Additional sampling from the positive carcase tested by FSIS discussed above (APHIS, 2024), included several different types of muscle tissues that correspond to common retail cuts of meat, and H5N1 influenza A virus was not detected. We are not aware of any studies of infected beef cattle or surveillance of beef herds for H5N1 to date (uncertainty).
The picture for offal may be more complicated. A study by Caserta et al. (2024) studied samples from dairy cattle from nine affected farms across four states in the USA. Results from rRT–PCR on tissues collected from three affected cows revealed the presence of viral RNA in the lung (viral titre 2.8 Log10 TCID50/mL), supramammary lymph nodes (viral titre 2.8 Log10 TCID50/mL) with the highest RNA levels in the mammary glands at a titre of between 7.3-7.8 Log10 TCID50/mL. At retail, samples of ground beef were tested where dairy herds, condemned at select FSIS-inspected slaughter facilities, have tested positive for H5N1. We have no information as to location of these slaughterhouses. No viral RNA was detected by PCR (APHIS, 2024). Of note, unlike bacteria, viruses are unlikely to be spread within the slaughter line unless they are present in fluids i.e. blood or milk. An animal that had systemic disease would likely be identified at the ante-mortem inspection by the Official Veterinarian.
Processing: effects on virus
Temperature and Time Parameters for Viral Inactivation (cooking/heating)
Beef is used in the production of ready meals. Around 0.3 million kg of beef sold in the UK every year is in the form of ready meals (AHDB, 2024). This production is likely to involve processing that will significantly reduce the levels of infectious virus present, as Regulation No 852/2004 on the hygiene of foodstuffs requires food business only place safe food on the market. There is no legislation that instructs businesses how to do this, but it will be covered by individual Hazard Analysis Critical Control Plans (HACCP). It is assumed that FBOs producing cooked foods, will follow this guidance (uncertainty).
Drying
Beef jerky and biltong are raw, dried, beef products. They are manufactured using a variety of drying techniques including freeze drying (at -55°C), ultrasonic vacuum drying using temperatures of 25-45°C; infrared drying requiring a temperature of 70°C and air drying; hot air drying requiring temperatures of 80°C and shade and sun drying at much lower temperatures of 15-20°C and 25-28°C respectively (He et al., 2023). We do not know how much of this type of product is produced in the UK (uncertainty).
Beef jerky undergoes post-drying processing to reduce microbial loads. Methods used include, pressure processing (HPP) with a reported process of two cycles of HPP treatment with 550 MPa at 21°C for 60 s (Yamamoto et al., 2017). Isbarn et al., investigated the effects of HPP treatment on HPAI H7N7 and reported that homogenised chicken meat suspended in culture medium inoculated with H7N7 at a level of 107 to 108 PFU/ml for 25 seconds at 15°C and 500 MPa induced a 5 log reduction in virus titres (Isbarn et al., 2007). It is likely that HPP treatment of beef jerky would significantly reduce any H5N1 present (uncertainty).
Minced beef
Although there is no evidence to confirm that AI is circulating in US beef cattle, approximately 6% of US beef originates from cull dairy cattle. In the US in May 2024, APHIS collected ground (minced) beef samples from retail outlets in the states in which dairy cattle herds have tested positive for H5N1 influenza virus. We have no information as to the number of samples tested (uncertainty). The samples were analysed using PCR to indicate whether any viral particles were present. No virus particles were found to be present. It is assumed that the mincing process will not affect the survival of virus in the meat.
Offal
A range of beef offal can be consumed, and numerous recipes can be found on the internet. The BBC food website contains recipes containing tongue, sweetbreads (thymus), tripe, oxtail, kidney and heart. Other websites contain recipes for calf liver and lung. Whilst the whole range of these offal types may not be routinely sold in supermarkets, they would be available to buy from butchers and farm shops or served in restaurants. It is unknown if beef offal is routinely added to beef burgers or beef sausages, but beef offal burgers are available at retail containing beef liver and beef heart. The FSAs flagship survey of consumer behaviour, “Food and You2” suggests that only 36% of consumers always thoroughly cook red meat although data on offal wasn’t specifically included it is assumed that similar trends will apply (FSA, 2022).
Retail: survival during shelf life
Beef and products containing beef are normally stored at chilled or frozen temperatures. Although there are no specific studies of this strain in beef or beef products, viruses survive longer at lower temperatures, and studies using poultry meat confirm that H5N1 is able to survive in muscle tissue for extended periods. In a small study by Yamamoto, Nakamura and Mase (2017), it was demonstrated that H5N1 could still be detected after 160 days at 4°C in poultry muscle, although viral titres decreased by between 2.0 and 3.7 Log10 EID50/ml. By 160 days there was no detectable virus. In the same study, they showed that virus could still be detected in poultry liver kept at 4°C for at least 20 days, although the titre decreased between 0.7 and 5.3 Log and virus was undetectable in all samples by day 30. This study went on to investigate the survival of H5N1 at 20°C – a temperature equivalent to ambient which products such as beef jerky would be kept. Virus in poultry muscle was detectable for up to 20 days but titre declined by between 1.8 and 4.5 Log and was undetectable by day 30.
Domestic processing
Raw consumption
Beef can be consumed raw in the form of beef tartare or carpaccio. If any viable virus were present in the beef, it could remain viable during the shelf life.
Cooking
Luchansky et al. (2024) experimentally measured the inactivation of H5N1 in beef burgers (“patties”) during cooking. They used 300g of meat (3 times higher than a “normal” burger) and spiked them with 5.6 Log10 EID50 per 300g H5N1 influenza A virus. Temperature was continuously monitored at 5-second intervals until the target internal temperature of the meat was achieved. Once achieved the meat was removed from the grill and within 2 minutes was placed in a water bath. Cooking to an internal temperature of 71.1°C (considered “well done” in this study and the FSIS recommended cooking temperature) took an average of 24 minutes and resulted in no virus being detected (at least 5.6 Log10 reduction). Even at a lower temperature of 62.8°C resulting in a “medium” cooked burger, cooked for an average of 22 minutes, no virus was detected either. The FSA advises cooking burgers to an internal temperature of 70 °C for 2 minutes (FSA, 2024).
Less than thoroughly cooked (LTTC) beef burgers
Luchansky et al., did consider LTTC burgers, cooking at 48.9°C which took around 15 minutes to reach temperature. Even at this low temperature a reduction in the titre of infectious virus was observed from 5.6 ± 0.4 Log10 EID50/300g in uncooked burgers to 3.1 ± 0.4 Log10 EID50/300g (2.5 Log reduction). The FSA advises domestic consumers not to produce LTTC burgers at home (FSA, 2024) however, data collected by “Food and You2” suggests that 31% of consumers will consume less than thoroughly cooked burgers at home. Whilst there is no legislation informing business as to the temperature that they must cook food to, it is the responsibility of businesses to place safe food on the market. For businesses wishing to sell LTTC burgers, a consumer message is required at the point of sale to help consumers understand the potential risks of eating LTTC beef burgers so they can make an informed choice when ordering. Guidance advice for businesses on production of LTTC burgers is based on experiments assessing the reduction of bacterial counts; methods they can use are discussed below:
Sous-vide cooking
Burgers are vacuum packed and cooked in a water bath for a longer period and at a lower temperature than conventional cooking resulting in a burger that looks “pink” but is in fact cooked. A validated time/ temperature combination equivalent to 70°C for two minutes must be achieved (FSA, 2024). Considering evidence from the study by Luchansky et al. (2024) this will significantly reduce any H5N1 present.
Sear and shave
The outer surfaces of a whole muscle piece of beef are sufficiently cooked to achieve at least a 6 Log reduction in bacteria, these are then shaved off and the remaining meat is minced and used to make burgers which are lightly cooked (FSA, 2024). We do not have any evidence as to the titre of H5N1 in infected beef cattle muscle (uncertainty) and we assume that an infected animal could have virus distributed throughout the muscle. Therefore, this method could result in survival of any H5N1 present depending on temperatures reached during cooking (uncertainty).
Source control
Beef, minced beef and beef burgers are produced with strict controls in place and the beef burgers are then lightly cooked to achieve at least a 4 Log reduction in bacteria. Steps to be taken at each stage of the food chain when using this method ensuring robust microbiological testing, strict hygiene measures and registration of businesses (FSA, 2024). Due to the differences in bacterial contamination vs viral infection, lack of surveillance of beef cattle in the UK and lack of evidence of clinical signs in beef cattle, these processes are unlikely to reduce the probability of infected cattle entering the food chain or the survival of H5N1 present in beef (uncertainty). Mitigation of the virus would depend on temperature reached during cooking.
Less than thoroughly cooked (LTTC) beef
Beef steak and joints can be consumed less than thoroughly cooked. There are currently no studies that we are aware of that have considered the survival of H5N1 during cooking of beef steaks or joints. Data collected by the FSA’s consumer behaviour study “Food and You2” suggest that 61% of consumers will occasionally eat “pink” red meat in the home and the number consumed at restaurants is likely high. The BBC food website suggests internal temperatures for different end points of steak with rare being 52°C, medium rare 55°C, and medium 60°C. The study by Luchansky et al., discussed above suggests that even at lower temperatures used for rare meat, H5N1 levels are reduced by 2.5 Log in burgers. It is assumed that the same level of reduction would be seen in beef steak and joints.
Consumption: potential for infection via ingesting virus
Data from the National Diet and Nutrition Survey (NDNS, 2021) indicates that beef and beef products (such as mince, beef fat, ready-made beef burgers) are consumed in higher amounts per portion than beef offal. Adults aged 19-64 have the highest mean intake of beef with a serving size of 110g, followed by adults aged ≥65 years at 91g, then children aged 11 – 18 at 88g suggesting that these groups are at highest risk of exposure through consumption of contaminated meat. Children under 3 years have lowest mean serving size of beef at 39g per portion suggesting that they have the lowest risk of exposure to H5N1 via consumption of contaminated beef. NDNS does not record individual data for pregnant women. Therefore, females in the 16-49 years age group are of childbearing age and thus acts as a proxy for pregnant women. These data indicated women aged 16-49 consumed an average serving size of 93g making them the second highest group in terms of mean serving size.
Adults aged ≥65 years group consume the largest serving of beef offal at a mean portion size of 23g per person per serving. Women aged 16-49 consume an average serving size of 22g making them the second highest consumer age group. Therefore, those consuming the highest mean portion size of beef offal are two groups potentially considered vulnerable to infections. Across all age groups the mean serving size of beef is 77.g and beef offal 15.6g.
There are numerous supplements available on the market that contain beef products. Examples of products with serving sizes are shown in Table 1.
Searches on commonly used websites such as Amazon show that multiple UK-produced supplements can be purchased. We do not know how many of these supplements are purchased in the UK per year (uncertainty). Marketing for these products is aimed at a particular demographic i.e. body builders and those wishing to follow a paleo diet. This limited data suggests the maximum consumed portion size is 3.6g per day (Table 1). We have no further data on the consumption of these beef product supplements (uncertainty).
Hazard Characterisation
Due to its recent emergence, limited information specific to HPAI clade 2.3.4.4b genotype B3.13 is available, and hazard characterisation will necessarily draw upon evidence relating to other strains, which will be reflected in the uncertainty assigned to our assessment.
Risk of AI infection from food
Although by far the most common transmission pathway for influenza virus to infect humans is via aerosol and droplet infections, experimental infections suggest that animals such as birds can contain very high viral titres in their tissues and internal organs post infection (up to 108.0 Log10 EID50, Thomas and Swayne, 2007). There is anecdotal evidence that the consumption of the uncooked blood, poultry meat, gamebirds or wild birds has transmitted HPAI H5N1 virus to carnivorous animals, including tigers (Hu et al., 2016), leopards (Keawcharoen et al., 2004) domestic cats (Kuiken, 2004), domestic dogs (Songserm et al., 2006), stone martens, (WHO, 2024), ferrets (Bertran & Swayne, 2014) and lions (Chen et al., 2016).
Reports of human infection are very rare. There have been isolated reports of individuals becoming ill after consuming infected uncooked animal products; in 2005 a 27-year-old Vietnamese woman became ill after she drank duck blood as part of a local dish. However, in this instance, other routes of transmission could not be ruled out (IATP, 2005). In 2006, the European Food Safety Authority (EFSA) Scientific Panel on Biological Hazards considered the risk of infection to humans from contaminated poultry and eggs and concluded that “there was no epidemiological evidence to date that avian influenza can be transmitted to humans through consumption of food” (EFSA, 2006).
The infectious dose of AI for humans is unknown. Several studies have investigated oral and intranasal inoculation of AI in animals (O’Brien et al., 2021). A study by Bertran and Swayne in 2014 in which ferrets were exposed to different HPAI viruses (H5 and H7 subtypes) through consumption of infected chicken meat, showed that the dose of virus needed to infect ferrets through consumption (108.9-109.2 EID50) was much higher than via respiratory exposure (107 EID50) and varied with the virus strain (Bertran & Swayne, 2014). A 2012 study by Reperant et al., showed that intragastric inoculation of domestic cats at a level of 107.8 TCID50 resulted in fatal systemic infection (Reperant et al., 2011). In 2011, Shinya et al showed that the inoculation of hamsters with H5N1 directly into the digestive tract at a level of 107.1-107.3 TCID50 allowed the virus to enter the bloodstream through the digestive lymphatic system (Shinya et al., 2011). It is unclear to what extent these dosages represent a biologically relevant risk of oral transmission. At present, there are no well-documented cases of human AI infection from food, where respiratory exposure could be completely ruled out (O’Brien et al., 2021). Collectively however, these results suggest that the oral infectious dose for humans is unlikely to be much lower than 107 TCID50.
Avian influenza and human health
Avian influenza infections in humans can present a wide spectrum of disease manifestations, ranging from mild to severe. Mild cases often resemble common flu symptoms, including fever, cough, sore throat, and muscle aches. Some individuals may experience conjunctivitis, which is an inflammation of the eye. Symptoms typically appear 3 to 5 days after infection. In more severe cases, avian influenza can lead to serious respiratory complications. Patients may develop pneumonia, acute respiratory distress syndrome (ARDS), and multi-organ failure. These severe manifestations can require hospitalisation and intensive medical care (NHS, 2024). The progression to severe disease is influenced by factors such as the specific strain of the virus, the patient’s age, underlying health conditions, and the timeliness of medical intervention. In rare instances, avian influenza infections can result in fatal outcomes. Higher mortality rates are associated with certain highly pathogenic avian influenza (HPAI) strains, such as H5N1 and H7N9. Infected cases may be given antiviral medicine such as oseltamivir or zanamivir, which may help reduce the severity of disease, prevent complications and improve the chances of survival (Smith, 2010).
Human cases of HPAI H5N1 linked to the most recent outbreak in the US
In April 2024, the WHO was notified of a human case of AI H5N1 in Texas. The individual, exposed to infected dairy cattle, developed conjunctivitis. Tests confirmed AI H5N1 clade 2.3.4.4b. The genotype was classified as B3.13, which was the same genotype detected in dairy cattle in Texas. The patient recovered after treatment with oseltamivir and no further cases were linked to this incident. In May 2024, two human cases were reported in Michigan. These unrelated cases were both dairy workers exposed to cattle infected with AI H5N1 clade 2.3.4.4b genotype B3.13. One had conjunctivitis, the other mild respiratory symptoms. Both recovered after treatment with oseltamivir, with no additional cases reported. In July 2024, A fourth case was reported in Colorado, a dairy farm worker exposed to infected cattle. This individual developed conjunctivitis, was treated with oseltamivir, and recovered (UKHSA, 2024).
The CDC have since reported that there are a total of 57 confirmed cases of HPAI H5N1 to date as a result of the most recent US outbreak; 34 cases have been linked to exposure from cattle, 21 from poultry, and 2 from unknown sources (CDC, 2024b).
UKHSA reports of H5N1
A proportion of infections with H5N1 may be asymptomatic. Since 2023, the UK Health Security Agency has received 4 positive human detections of AI H5N1 clade 2.3.4.4b in exposed persons on farms in England where AI H5N1 was also confirmed in the poultry on site. 144 individuals from 8 infected premises have been tested, of which 4 were positive (2.7%). All detections were identified as part of an ongoing enhanced surveillance study of asymptomatic workers exposed to premises infected with AI. It remains unclear whether the detections in these asymptomatic individuals reflected deposition of viral particles on the mucosal surface (in other words, not causing infection) or infection with active viral replication (uncertainty) (UKHSA, 2023).
Global reports of H5N1
Symptomatic human cases of AI H5N1 continue to be detected globally, including cases of clade 2.3.4.4b. Since 2023, prior to the latest human cases in the USA associated with exposure to infected dairy cattle, detections in humans either confirmed to be, or associated with, clade 2.3.4.4b viruses have been reported in Ecuador, China and Chile. These cases were not fatal but did develop severe disease requiring hospitalisation (UKHSA, 2024).
Vulnerable groups
Vulnerable groups vary by strain for influenza. Limited information for B3.13 is available as it is a newly emerging strain. Different groups will be vulnerable to different strains (uncertainty).
Risk characterisation
The infectious dose for H5N1 for humans via ingestion has been hypothesised to unlikely be much lower than 107 TCID50 and there is still only very limited evidence of humans becoming infected with avian influenza from food. We do not know the titre of infectious virus in the muscle of beef from cattle infected with avian influenza A (H5N1) clade 2.3.4.4b genotype B3.13.
Two separate FSIS studies have investigated the potential presence of H5N1 viral RNA in muscle tissue from dairy cattle as part of a programme of surveillance in states where virus was known to be circulating, each with a distinct focus and sampling approach. The first focused on condemned animals at slaughter facilities, where one out of 109 muscle samples tested positive for H5N1 viral RNA at very low levels. The second, part of the FSIS’s broader surveillance program launched in September 2024, involved routine testing of culled dairy cows regardless of clinical signs. Only one muscle sample tested positive for H5N1 viral RNA (APHIS, 2024). These findings suggest that the low detection rates likely reflect a low prevalence of infection among sampled animals. However, because the sampling was not targeted specifically at farms or regions where virus was known to be circulating, the prevalence on infected farms is likely to be higher. Additional sampling from one of the carcases, including several different types of muscle tissues that correspond to common retail cuts of meat, did not detect infectious virus or viral particles. In beef offal, H5N1 has been detected in the lung at a titre of 2.8 Log10 TCID50/mL and mammary glands at 7.3-7.8 Log10 TCID50/mL. In the UK there are robust systems at slaughterhouses to ensure that animals that are not fit for consumption are detected and removed from the food chain. It is likely that any animal with clinical signs, and thus with a high viral load, would be detected via these routes and not enter the food chain.
Thoroughly cooked beef, minced beef and beef offal
If meat from infected cattle did enter the food chain, H5N1 is susceptible to heat treatment. A temperature of 63°C and above has been shown to inactivate infectious virus in beef that was inoculated with high titres (at least 5.6 Log), and this is likely much higher than would be seen in a natural infection.
Therefore, the probability that UK consumers will receive infectious exposures to influenza of avian origin via a portion of thoroughly cooked beef and minced beef contaminated with avian influenza A(H5N1) clade 2.3.4.4b genotype B3.13 is considered to be Negligible. The uncertainty in this estimate is Low, as we have evidence that H5N1 is eliminated by thorough cooking. “Low” is defined as “There are solid and complete data available; strong evidence is provided in multiple references; authors report similar conclusions”.
Less than thoroughly cooked beef, minced beef and offal
Businesses that provide less than thoroughly cooked minced beef must adhere to processes that are designed to reduce the bacterial load of the meat. Some of these are unlikely to mitigate risk of virus and do not apply to consumers making their own LTTC burgers at home. The guideline temperature for beef to be cooked rare is 52°C and would also apply to LTTC burgers and offal. Cooking to a temperature of 49°C, significantly reduces infectious virus load (2.5 Log reduction). Even considering lung tissue and mammary tissue, where viral titres have been quantified these temperatures would be sufficient to reduce the virus significantly.
The probability that UK consumers will receive infectious exposures to avian influenza A(H5N1) clade 2.3.4.4b genotype B3.13 via a portion of less than thoroughly cooked beef, burger and offal is considered to be Negligible (so rare it does not merit to be considered), due to the heat treatments used to produce such foods, whilst not as extreme as in thoroughly cooked foods, is still apparently sufficient to reduce viral titres.
The uncertainty in this estimate is Medium, due to the lack of evidence on the distribution and titre of the virus in beef muscle and offal and the variations in processes and temperatures used to produce less than thoroughly cooked foods. “Medium” is defined as “There are some but no complete data available; evidence is provided in a small number of references; authors report conclusions that vary from one another.” As the uncertainty is “Medium” and this is a rapidly evolving situation, any new evidence that may require this rapid risk assessment to be updated will be actively monitored.
Raw beef
Studies have shown that the virus can survive up to 160 days at 4°C in poultry muscle, although viral titres decreased by between 2.0 and 3.7 Log10 EID50/mL during this time. Products such as beef carpaccio and beef tartare undergo no further processing that we feel would mitigate any virus present and therefore if avian influenza A (H5N1) clade 2.3.4.4b genotype B3.13 were present in an animal then consumer exposure could occur. The probability that UK consumers will receive infectious exposures to avian influenza A (H5N1) clade 2.3.4.4b genotype B3.13 via a portion of raw beef products such as carpaccio and beef tartare is considered to be Very Low. "Very low, is defined as “very rare but cannot be excluded”.
The uncertainty in this estimate is Medium, due to the lack of evidence on the distribution and titre of the virus in beef muscle. “Medium” is defined as “There are some but no complete data available; evidence is provided in a small number of references; authors report conclusions that vary from one another.” As the uncertainty is “Medium” and this is a rapidly evolving situation, any new evidence that may require this rapid risk assessment to be updated will be actively monitored.
Severity of infection
In the event of infection, the severity of detriment is assessed as Low. Recent data from the CDC indicates there have been multiple confirmed human cases of HPAI (H5N1) linked to dairy cattle, with symptoms ranging from mild conjunctivitis to mild respiratory symptoms. As of November 2024, there have been 34 human B3.13 cases associated with cattle (CDC, 2024b). There may be underreporting for mild infections. Most of the human cases were in farm workers; hence, the CDC suggests those who have job-related exposure to dairy cattle, are at a greater risk of contracting HPAI virus (CDC, 2024a). “Low” is defined as "Mild illness: not usually life-threatening, usually no sequelae, normally of short duration, symptoms are self-limiting (e.g., transient diarrhoea). The assumption that the currently circulating strain does not commonly result in severe infection is based on the observation that if someone is severely affected by an influenza-like illness in the US they would normally report to medical professionals and be hospitalised and tested. There is therefore some level of confidence that this strain is not resulting in large numbers of severe infections to date.
The uncertainty in this severity is Medium which reflects the recent emergence of this strain, the limited clinical data on infection with this strain so far, and the fact that reporting disincentives make it difficult to be certain that other human infections have not occurred. Additionally, foodborne exposure has not been confirmed and it is unknown whether severity of illness is any different compared to other routes of exposure e.g., inhalation. “Medium” uncertainty is defined as “There are some but no complete data available; evidence is provided in small number of references; authors report conclusions that vary from one another”.
This document specifically assesses the risk from the strain involved in the current outbreak in US dairy cattle. Strains of influenza vary widely in their clinical presentation in infected humans. However, the majority of human cases of influenza of avian origin have been associated with Asian genotypes or clades. For influenza of avian origin as a whole (in this case, ingested via poultry products), the severity is considered to be High with Medium uncertainty (Kintz et al., 2023).
Key uncertainties
-
Data on the distribution and titre of virus in muscle tissue of infected beef cattle.
-
Data on the distribution and titre of virus in offal of infected beef cattle.
-
Effectiveness of processes used in production of LTTC burgers and other less than thoroughly cooked beef and offal in mitigating virus.
-
The severity of detriment is assessed as Low based on no evidence of severe illness and no vulnerable groups identified.
-
There has also been no confirmation that severity of illness from foodborne exposure is any different compared to other routes of exposure such as inhalation.
Abbreviations
Article updated on 21st August 2025