As part of the FSA’s responsibility for ensuring that food is safe we occasionally assess scenarios such as this one where a hazard does not yet occur in the UK, to ensure that we are better prepared in the event of an introduction.
Executive summary
Since the first confirmed case on 25th March 2024, Highly Pathogenic Avian Influenza A (H5N1) clade 2.3.4.4b genotype B3.13 has been detected in dairy cattle across the United States. During the outbreak, the American Food and Drug Administration (FDA) found viral RNA in about 20% of tested dairy products from retail stores. However, no infectious virus was detected in any of the samples. There is no evidence to suggest this virus is currently present in the UK or other European countries, and it has not been detected in UK cattle. This assessment sets out the risk to UK consumers in a hypothetical scenario where they are exposed to the virus as a result of consuming milk and dairy products from cattle herds, if the virus began circulating in UK cattle. This includes both pasteurised and unpasteurised cow’s drinking milk, milk and dairy products, as well as colostrum and colostrum-based products. The available evidence suggests that the virus is susceptible to heat treatment, and normal pasteurisation methods (Low Temperature Long Time and High Temperature Short Time) have been shown to reduce live infective virus in milk by 4.44 log to more than 6 log. Therefore, this assessment determined that the probability of individuals being exposed to an infectious dose of H5N1 virus from pasteurised milk, pasteurised colostrum or dairy products made from pasteurised milk was Negligible, on a per portion basis. This probability of exposure was given a Medium level of uncertainty.
However, UK consumers in England, Wales and Northern Ireland can purchase raw cow’s drinking milk (RCDM), and raw colostrum and dairy products made from unpasteurised milk can be sold throughout the UK. A typical portion of RCDM from a hypothetically infected UK cattle herd was assumed to contain a high level of infectious virus, as much as 8.5 Log10 EID50 infective viral particles per 150ml of milk. Under this assumption the probability of individuals being exposed to an infectious dose via RCDM was Medium, on a per portion basis. There were no available data on the levels of infective virus in raw colostrum, so it was assumed to be the same as RCDM. Additionally, there were significant gaps in the evidence available on the effect of producing dairy products (cheese, yoghurt, cream, butter and ice-cream) from milk containing the Influenza A(H5N1) virus, and therefore the effect of these processes on viral levels in the foodstuff is not certain. Thus, applying precautionary approach, the assessment determined that the probability of individuals being exposed to an infectious dose per portion of dairy products made with unpasteurised milk to be Medium also.
The probability of exposure per portion of RDCM, raw colostrum and dairy products made with unpasteurised milk was assessed to be with High Uncertainty, due to the lack of confirmed cases of H5N1 avian influenza that have been traced back to food consumption, and significant uncertainty around the amount of virus that would be required to be consumed to cause infection.
In the event of infection, the severity of detriment has been determined as Low. This is due to the fact that the only confirmed human cases of HPAI H5N1 (clade 2.3.4.4b genotype B3.13) infection, to date, have been mild cases in American farm workers who were in close contact with infected cattle. However, this is given with a Medium level of uncertainty as foodborne exposure has not been confirmed and it is unknown whether severity of illness will be different compared to other routes of exposure such as inhalation.
Statement of purpose
The purpose of this assessment is to understand the risk to the health of UK consumers from drinking milk, milk products, colostrum and colostrum-based products both pasteurised and unpasteurised (including thermised products), specifically the risk per portion of product in an area of infection, in the hypothetical scenario of an outbreak of HPAI H5N1 strain B3.13 in the UK.
Risk question
Given that Highly Pathogenic Avian Influenza virus (H5N1) has been detected in dairy cattle across the US, what is the risk of H5N1 to UK consumers from the consumption of the dairy products listed above if the virus was to be detected in UK dairy herds?
Hazard identification
The hazard considered for this assessment is an influenza A virus of avian origin classified as B3.13. Influenza viruses are negative-sense, single-stranded, enveloped RNA viruses classified in the family Orthomyxoviridae, and 80-120nm in diameter. Analysis of available sequences supports the hypothesis of a single bird-cow crossover event followed by cow-cow spread (ASTHO, 2024).
To date, there is no evidence to suggest Avian influenza A(H5N1) clade 2.3.4.4b genotype B3.13 is currently present in the UK or Europe (HAIRS, 2024).
Since the first confirmed case on 25th March 2024, a number of dairy herds in the US were reported as exhibiting clinical signs including inappetence and milk drop. 10-15% of animals on affected farms showed clinical signs, with minimal deaths. At sites in Texas, deaths of wild birds (pigeons, blackbirds, and grackles) and domestic cats, assumed to have consumed unpasteurised milk, were also reported (APHIS, 2024).
Although regional diagnostic labs were initially unable to identify a cause, samples received at the Iowa State University Diagnostic Laboratory in Ames on 24 March 2024 (Texas) and 25 March 2024 (Kansas) were found to be positive for influenza A virus (IAV) by PCR. A press release was issued on 25 March 2024 (APHIS, 2024) and an early-access manuscript fully describing these results was published on 29 April 2024 (Burrough, et al., 2024). The first confirmed case of this outbreak was on the 25th March 2024; sequence analysis raises the possible crossover to cattle could have occurred earlier (Science.org, 2024)
On 25 April 2024, the FDA reported that PCR testing on samples from a nationally representative commercial milk sampling study found influenza virus RNA in around 20% of retail samples tested, although the number of samples tested was not given (FDA, 2024b). On 26 April 2024 the FDA reported some preliminary results suggesting that pasteurisation is effective at eliminating infectious HPAI from milk (FDA, 2024b).
Since its detection the outbreak has continued to spread. Several routes have been proposed as possible mechanisms for spread between farms and to other states (Tomlinson, 2024). These include the movement of infected animals, the movement of contaminated milking equipment, and spread via wild birds (Burrough, et al., 2024). There are currently no national restrictions on cattle movement in response to this outbreak, however in April 2024 the US passed a federal order requiring mandatory testing and reporting for HPAI for the interstate Movement of dairy cattle.
The Animal and Plant Health Inspection Service (APHIS) has established a page linking to the latest updates on the situation at Highly Pathogenic Avian Influenza (HPAI) Detections in Livestock | Animal and Plant Health Inspection Service (usda.gov), which also includes a regularly updated map of states that have detected the current strain of influenza in livestock.
Exposure assessment
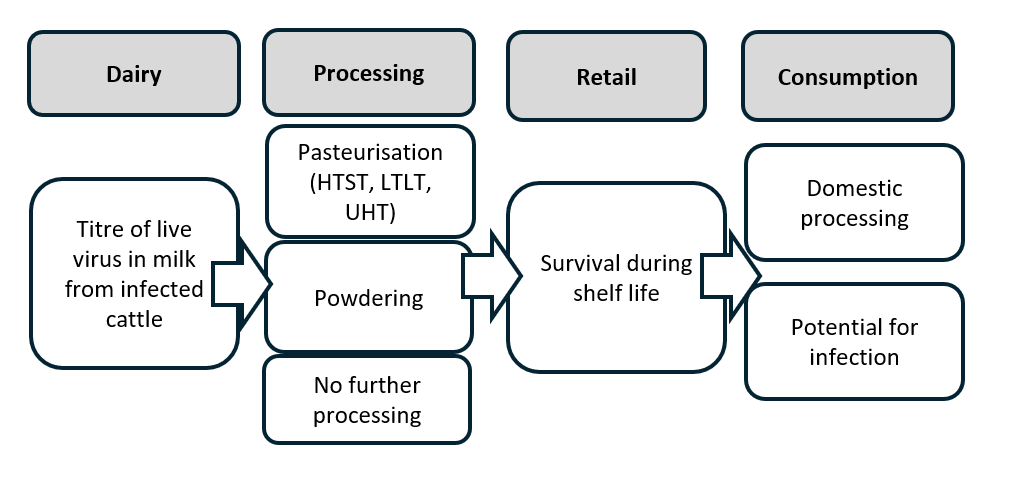
Risk Pathway

Dairy: titre of virus in milk from infected cattle
In the US unpasteurised milk shows high levels of viral nucleic acid, meaning a low Ct (cycle threshold) value in a PCR test. The lowest Ct value reported is 12.3 (Burrough, et al., 2024). The presence of viral nucleic acid alone does not necessarily reflect the presence of infectious virus, although the presence of some live virus in these raw milk samples has been confirmed. In a worst-case scenario, the quantity of viral RNA that would result in Ct value of 10 would be around 108.5log10 infectious virus particles per ml of milk.
The FDA, in collaboration with four states, tested unpasteurised milk samples from bulk tanks (capacity to hold milk from 600 to 700 cows), collecting from both affected and unaffected farms in regions with confirmed infections. These samples are collected routinely as part of procedures under the Pasteurised Milk Ordinance. Out of 275 raw milk samples tested using quantitative reverse transcription PCR, 158 (57.5%) were positive. Of the positive samples, 39 (25% of PCR-positive, or 14% of the total) contained infectious virus, with titres ranging from 1.3 to 6.3 Log10 EID50/mL, and a median titre of 3.5 Log10 EID50/mL. Authors noted that there was no strong correlation between the viral titre estimated from the PCR result and the amount of viable virus detected (R2 = 0.37) (Spackman et al., 2024).
Commercial Processing: effects on virus
Raw milk
Raw cow’s drinking milk (RCDM), which is not subjected to heat treatment, presents a potential exposure risk. In the UK, the sale of RCDM is permitted in England, Wales, and Northern Ireland, but it is prohibited in Scotland. Legal sales are restricted to direct transactions with consumers through registered milk RCDM production farms, farmers’ markets, direct online sales, or vending machines located at the farm (FSA, 2020). Recent studies have indicated that raw milk contaminated with the H5N1 virus, when stored at 4°C for five weeks, exhibits only a minor reduction in viable virus levels. This finding suggests that the H5N1 virus can remain infectious in raw milk under refrigerated conditions (Nooruzzaman et al., 2024). Moreover, dairy products can be made with unpasteurised milk. These products can include, but are not limited to, ice cream and butter. The volume of raw milk and raw milk products sold in the UK are unknown (uncertainty).
Pasteurisation
Pasteurisation is a process that involves heating milk to a high temperature followed by rapid cooling before it is bottled or packaged, to ensure safety to the consumer by eliminating harmful bacteria present in the milk as well as extend shelf life. Different temperature-time combinations are permitted, with the holding time being that required to achieve a specified reduction in the titre of the most heat-resistant microorganism typically found in the foodstuff at the indicated temperature. For milk, this is a 5-log reduction in the numbers of Coxiella burnetii (Codex & FAO, 2011).
In the UK, milk is normally pasteurised using one of the following three methods:
High Temperature Short Time (HTST) is a continuous method in which milk is heated to 71.7°C for 15 seconds. It is used for large scale processing of liquid dairy products and is commonly used for drinking milk.
Low Temperature Long Time (LTLT) is a batch method in which milk is heated to 63°C for 30 minutes. It is commonly used for small batch pasteurisation, for example as part of the on-farm production of dairy products such as ice cream.
Ultra-High Temperature (UHT), which involves heating the milk to at least 138°C for at least 2 seconds.
In addition, US regulations permit three further temperature-time combinations: 89°C for a minimum of one second, 96°C for a minimum of 0.05 seconds, or 100°C for a minimum of 0.01 seconds (IDFA, 2024).
To evaluate the effectiveness of pasteurisation in mitigating the risk of virus contamination in milk, a study spiked milk with 6.3 Log10 EID50/mL of clade 2.3.4.4b H5N1 virus (Alkie et al., 2025). This is the highest titre found in raw bulk milk tank testing (Miller, 2022; Spackman et al., 2024). After LTLT pasteurisation no infectious virus could be detected (>6 Log reduction). After HTST pasteurisation no infectious virus could be detected in seven out of eight experimental replicates (>6 Log reduction). In one replicate, a 4.44 Log virus reduction was achieved, which would be sufficient to eliminate the typical viral quantities detected in bulk milk from affected areas. There are no data available on whether the other permitted temperature-time combinations are effective.
In May 2024, Schafers et al., published findings on the effectiveness of pasteurisation on inactivating influenza A viruses in cow’s milk. They found that commercial pasteurisation conditions, LTLT: 62.5°C for at least 30 minutes, and HTST: 72°C for at least 15 seconds, rapidly inactivated influenza A type viruses and reduced the titre of infectious virus from ~107 PFU/ml to below the LoD, 33 PFU/ml (~5-6 Log reduction) in all instances. Infectivity of HPAI H5N1, as assessed in egg haemagglutination assay found that while viral genetic material remained detectable after pasteurisation, no infectious virus was recovered from pasteurised milk (Schafers et al., 2024).
In July 2024, Franziska Kaiser, in a letter to the editor of the NEJM reported similar findings using raw cow’s milk spiked with the virus to 106 TCID50/mL HPAI A(H5N1) virus A. At 63°C they found that virus inactivated from 106 TCID50/mL to undetectable levels within 2 minutes. (Estimated half-life of infectious virus: 4.5 seconds). At 72°C, the virus titre decreased from 105 TCID50/mL to 101 TCID50/mL within 5 seconds. Very low titres (<101 TCID50/mL) were detected until 20 seconds; no viable virus was found at later time points (Kaiser et al., 2024).
In June 2024, Cui et al., published findings on the thermal stability of Influenza A viruses, including H5 clade 2.3.4.4b viruses. They found that submitting milk containing virus at titres of ~107 EID50/mL to 63°C for 30 minutes or 72°C for 15 seconds achieved a complete inactivation of H5N1 viruses, corresponding to a reduction of around 106.5 EID50/mL as measured in an embryonated chicken egg viral assay (Cui et al., 2024).
Caceres et al., investigated the stability of the virus in commercially available pasteurised whole milk, spiked with 8 Log10/mL virus, under various thermal conditions. Heat treatment at 63°C for 30 minutes effectively reduced viral viability below the limit of detection (1 Log10 TCID50/mL) representing at least a 7 Log reduction in viral titre. At 72°C for 20 seconds, the reduction in viral titre was inversely proportional to the volume of sample that was heat treated. Significant reductions in virus were observed in the smallest volume (2 µl, 6 to 7 Log reduction) but little or no reduction was seen in the largest of the sample volumes tested (200 µl, <1 Log reduction). Treatment at 91°C for 20 seconds resulted in larger reductions in viral titre than 72°C for 20 seconds, but again the reduction was inversely proportional to sample volume. It is unclear why these findings are in contradiction to other similar studies or why efficacy of pasteurisation is inversely related to sample size (Caceres et al., 2024).
Powdered milk products
There are three common methods for producing powdered milk (Miller, 2022). These consist of:
-
Spray Drying - milk is first flash-pasteurised to kill any bacteria. It’s then reduced to around 50% of its original mass by steaming, separating the vapour from the powder and condensing it to a liquid which is removed. The milk is then sprayed into a drying chamber, exposing it to hot air. The liquid milk droplets quickly evaporate, leaving behind a dry powder.
-
Drum Drying - a faster method that involves passing the milk over a thin film on a heated drum which steams the milk, leaving solids behind which are extracted and ground into a fine powder. Of the three methods listed here, drum drying is the least used as it can caramelise the milk.
-
Freeze Drying - freeze drying is complex and expensive and involves slowly freezing the milk at -50°C to -80°C. Milk is then subjected to low heat and low pressures in a partial vacuum, which helps a process called sublimation turning ice from solid state to gas. The gas is then condensed and collected, leaving behind a dry powder.
It is highly likely that the first two methods would inactivate any virus present in milk, although the effect of the final method is less certain.
On 26 April 2024 the FDA published a statement that PCR testing of “several” powdered infant and toddler formula samples came back negative (FDA, 2024a). The statement does not specify the number of samples tested (although they were a subset of “an initial limited set of geographically targeted samples” collected as part of a national commercial milk sampling study in coordination with UDSA). The statement also does not state which of the aforementioned processing methods was used.
In conclusion, although there are limited direct studies of the effects of the commonest forms of pasteurisation (HTST and LTLT) on the inactivation of influenza virus of avian origin, those that do exist suggest that it significantly reduces the titre of infectious virus present and thus mitigates the risk to some extent, although it does not always eliminate all infectious virus present. By extension it is probably reasonable to assume that other temperature-time combinations permitted for pasteurisation would be similarly effective.
Survival characteristics of H5N1
Shahid et al. (2009) assessed the effects of different physicochemical parameters including pH on the survival of H5N1. They observed that H5N1 lost infectivity when exposed to pH 1, 3, 11 and 13 after 6 h and remained infective at pH 5 (for 18 hours) and p H 7 and 9 (for more than 24 hours). A study of the environmental survival of avian influenza virus in water at different pH and temperatures found that all the AI viruses tested in the study were, in general, most stable at pH 7.4-8.2 and at lower salinities (< 2%) (and at lower temperatures of 17°C) (Brown et al., 2009), while a study by Keeler et al. (2014) showed that AI virus persisted in waters at temperatures <17°C, that had a neutral to basic pH of 7.0-8.5, and a low salinity of less than 0.5 parts per thousand (ppt) (equivalent to 0.1%) (Keeler et al., 2014). The pH of raw milk can vary based on animal breed, diet, and stage of lactation but typically ranges between 6.4 and 6.8 (safemilklabs, 2025). Specific manufacturing processes involved in the production of milk products alter the pH (details below).
Dairy product processing in the UK
A variety of dairy products are manufactured and sold in the UK. These products can be made with pasteurised or unpasteurised milk. The rate at which a virus is inactivated in dairy products depends on the production process, storage conditions, and physicochemical characteristics (Possas et al., 2021). Key factors include milk heat treatment (e.g. pasteurisation), pH, salinity, and storage temperature.
Cheese
Most cheese in the UK is pasteurised. However, some cheeses, like Stichelton, are always made with raw milk (SCA, 2024). However, some cheese may be manufactured from either unpasteurised or pasteurised milk. Cheddar, the most consumed cheese in the UK (over 50% of cheese market), is an example as it is typically made from pasteurised milk, but some producers of artisanal Cheddar cheeses make it with raw milk (Amanatidou et al., 2024).
The physicochemical properties of cheese, such as pH, water activity (aW), and salt content, vary widely. For instance, pH ranges from 3.9 in Skyr to 6.8 in Roquefort (Amanatidou et al., 2024), while aW varies from 0.858 in hard cheeses like Grana Padano to 0.99 in whey cheese. Salt content also differs significantly, from 5.5% in Romano to less than 0.5% in ricotta (Fox et al., 2017). Therefore, assessing viral survival and infectivity in cheese is complex and should consider a range of potential factors.
Studies have shown that cheese processing methods, such as pressing and heat treatment, can reduce virus levels. For example, a study by Cliver, (1973) showed influenza A in cheddar cheese was reduced by over 4 Log after pressing. Even when raw milk is used, processes like heating and stretching (commonly to 70-80°C in mozzarella production) and brining (with 10-18% NaCl in cheeses like feta) can reduce virus survival (Gonçalves & Cardarelli, 2021). Ripening periods, which vary from none in cottage cheese to over two years in Parmesan, also affect pH (Amanatidou et al., 2024). During ripening and other processes cheeses usually undergo acidification due to the addition/ presence of Lactic acid bacteria, resulting in an acidic pH level (Cheddar, Parmesan, and Gouda) (Amanatidou et al., 2024).
As previously mentioned, an acidic pH can impact H5N1 infectivity. However, the extent to which viral inactivation occurs in different cheese types made with unpasteurised milk remains uncertain (uncertainty). Additionally, unripened cheeses, with high moisture and low salt content, do not undergo these pH changes.
Yoghurt
Yoghurt is produced by fermenting milk with lactic acid bacteria. Fermentation results in the production of lactic acid, lowering the pH to 4.0-4.6 (Ayivi, 2022). A study by Lang et al. (2024) investigated the survival of H5N1 viruses in homemade dairy products. They found viral RNA in yoghurt samples, although no viable virus was detected. The authors suggest that the acidic pH contributes to the loss of virus infectivity. Therefore, it is possible dairy products with lower acidic levels may reduce the infectivity of the virus, but no data is available (uncertainty).
Butter and cream
The production of cream typically involves centrifugal separation, where milk is spun rapidly in a centrifuge. This process separates cream from the milk and reduces liquid volume as the cream is extracted. Cream generally has a low salt content unless specifically salted, and usually has a slightly acidic pH to maintain stability and flavour (pH 6.4 to 6.7) (Lim et al., 2022). Butter production typically involves ripening cream by adding bacterial cultures, which can lower the pH (range from 4.5 to 6.0) (McDowell, 1964). Ripened cream is then churned, separating buttermilk from the liquid (Kishan, 2018). Salt may also be added to preserve and flavour, and salinity typically ranges around 1.5%.
Ice-cream
The production of ice-cream typically begins with combining liquid ingredients and heating to approximately 43°C (length of heating period not specified). Therefore, infectivity of the virus may occur (uncertainty). This heating can be followed by further pasteurisation and homogenisation under high pressure to break down fat. Throughout the processes, ice-cream typically maintains a nearly neutral pH (around 6 to 7) . Therefore, processing used in dairy product production varies, resulting in a range of physiochemical properties that may alter the infectivity of the virus. However, there is no data available explicitly testing the viability of the virus in different dairy products (uncertainty).
Retail survey results
Furthermore, a retail sample survey (FDA, 2024b) in the US tested a variety of dairy products from multiple retail locations for live virus and viral RNA. This sampling was conducted between 18 June and 31 July 2024. Out of 167 samples, none tested positive for viable H5N1, while 17% (29 samples) were positive for viral RNA. Skim milk, heavy cream, cream cheese and aged raw cheese had no viral RNA detected. Viral RNA was detectable in a small to moderate proportion of whole, 1%, and 2% milk (4.3% to 18.3%), and could be detected in 14.3-16.7% of cheddar and processed cheese. Viral RNA was detected in a higher proportion of mozzarella cheese, butter and ice cream (40.9% to 50%), although the number of samples of each product tested was small. The non-detection of viral RNA in products such as raw milk is likely due to the milk not being contaminated, rather than the result of processing, considering the other results presented above. On 21 November 2024 the California Department of Public Health announced a recall of whole raw milk after testing had confirmed the virus was present. Therefore, it can be assumed that dairy products made and sold in the UK will undergo similar methods of production as US products; thus, similar levels of viral infectivity and deactivation may occur (uncertainty).
Milk products made with unpasteurised milk
Typically, commercial milk products such as cheese, yoghurt, cream, butter and ice cream are pasteurised, reducing the risk of exposure to viable virus via consumption.
However, in the UK, the sale of raw milk products such as cream, ice cream and yoghurt (list not exhaustive and other products may be available) is legal but restricted to registered food businesses (FSA, 2020). To protect consumers, producers of dairy products made with raw milk must comply with dairy hygiene rules and microbiological standards. Compliance with these requirements is monitored through risk-based inspections. The volume of unpasteurised milk and milk products sold to consumers in the UK is not currently known (uncertainty).
Colostrum and colostrum-based products
Colostrum is the first form of milk that is released by mammary glands after birth and has a pH of 6.4 (Puppel et al., 2019). There have been incidents of cats with respiratory and neurological signs from HPAI affected dairy farms in the US (Burrough, et al., 2024). These incidents are believed to have resulted from the consumption of raw milk or colostrum. Bovine colostrum can be used in preserved forms such as powder, liquid, tablets, or capsules as dietary supplements. Processing methods such as thermal treatment are used to produce the different forms of bovine colostrum to comply with food safety regulations (Kaplan, 2022). Thermal processing (including HTST and LTLT) have been shown to effectively inactivate the virus. However, colostrum can be sold raw directly from farms, similar to raw milk; the volume of colostrum for human consumption on the UK market is not currently available but the volume is likely to be low due to low production volumes and shorter collection periods (Godden et al., 2019) (uncertainty). The level of viral viability in raw colostrum is assumed to be similar to raw milk (uncertainty).
Retail: survival during shelf life
Dairy products such as milk and cheese are often stored at chilled temperatures. In general, viruses are inactivated more slowly at chilled and frozen temperatures. A study by (Nooruzzaman et al., 2024) stored milk from infected cows at 4°C (refrigerator temperature) and observed a reduction in infectious virus from 5.97 Log10 TCID50/mL on day 0 to 2.05 Log10 TCID50/mL after 42 days, with virus still detectable after 56 days. Therefore, virus present in milk or dairy products may persist at refrigeration temperatures for weeks or months. Virus which survives the freeze-drying process can persist very well at ambient storage temperatures.
Surveillance data indicates that HPAI viruses, such as H5N1, can persist in frozen duck meat (Chmielewski and Swayne, 2011). This persistence suggests that virus which is not inactivated during the production of frozen dairy products such as ice-cream could persist for prolonged periods (uncertainty).
Consumption
Domestic processing
Consumers often process dairy products in various ways, such as grilling or incorporating them into sauces. These methods typically involve heating the products to high temperatures, which is likely to inactivate the virus. However, these products are also often consumed without further processing, so to yield a conservative estimate of risk we do not consider consumer processing guaranteed to reduce the probability of exposure.
Consumption of dairy products
Consumption of unpasteurised dairy products with viable virus is a potential exposure risk. Additionally, the volume of raw drinking milk and products made with unpasteurised milk consumed is unknown (uncertainty). Data from the National Diet and Nutrition Survey (NDNS, 2021) indicates that cow’s milk is the dairy product consumed in the highest amount per portion (compared to cheese, milk powder, whey powder, yoghurt and ice cream). Consumption of cow’s milk varies across different age groups. Individuals under 65 years of age consume on average 80 to 150 grams of cow’s milk per serving. The average serving by age group: Infants (4-18 months)-110 grams, Toddlers (1.5-3 years)-150 grams, Children (4-10 years)-150 grams, older children (11-18 years)- 140 grams and Adults (19-64 years)-80 grams. The elderly (≥65 years) have lower mean intakes of cow’s milk (69 grams), indicating a reduced exposure risk.
Hazard characterisation
Due to its recent emergence, limited information specific to HPAI clade 2.3.4.4b genotype B3.13 is available, and hazard characterisation will necessarily draw upon evidence relating to other strains, which will be reflected in the uncertainty assigned to our assessment.
Risk of AI infection from food
Although by far the most common transmission pathway for influenza virus to infect humans is via aerosol and droplet infections, experimental infections suggest that animals such as birds can contain very high viral titres in their tissues and internal organs post infection (up to 108 Log10 EID50, Thomas and Swayne, 2007). There is anecdotal evidence that the consumption of the uncooked blood or poultry meat, gamebirds or wild birds has transmitted HPAI H5N1 virus to carnivorous animals, including tigers (Hu et al., 2016), leopards (Keawcharoen et al., 2004) domestic cats (Kuiken, 2004), domestic dogs (Songserm et al., 2006), stone martens, (WHO, 2024), ferrets (Bertran & Swayne, 2014) and lions (Chen et al., 2016).
Reports of human infection are very rare. There have been isolated reports of individuals becoming ill after consuming infected uncooked animal products; in 2005 a 27-year-old Vietnamese woman became ill after she drank duck blood as part of a local dish. However, in this instance, other routes of transmission could not be ruled out (IATP, 2005). In 2006, the European Food Safety Authority (EFSA) Scientific Panel on Biological Hazards considered the risk of infection to humans from contaminated poultry and eggs and concluded that “there was no epidemiological evidence to date that avian influenza can be transmitted to humans through consumption of food” (EFSA, 2006).
The infectious dose of AI for humans is unknown. Several studies have investigated oral and intranasal inoculation of AI in animals (O’Brien et al., 2021). A study by Bertran and Swayne in 2014 in which ferrets were exposed to different HPAI viruses (H5 and H7 subtypes) through consumption of infected chicken meat, showed that the dose of virus needed to infect ferrets through consumption (108.9-109.2 EID50) was much higher than via respiratory exposure (107 EID50) and varied with the virus strain (Bertran & Swayne, 2014). A 2012 study by Reperant et al., showed that intragastric inoculation of domestic cats at a level of 107.8 TCID50 resulted in fatal systemic infection (Reperant et al., 2011). In 2011, Shinya et al showed that the inoculation of hamsters with H5N1 directly into the digestive tract at a level of 107.1-107.3 TCID50 allowed the virus to enter the bloodstream through the digestive lymphatic system (Shinya et al., 2011). It is unclear to what extent these dosages represent a biologically relevant risk of oral transmission. At present, there are no well-documented cases of human AI infection from food, where respiratory exposure could be completely ruled out (O’Brien et al., 2021). Collectively however, these results suggest that the orally infectious dose for humans is unlikely to be much lower than 107 TCID50.
Avian influenza and human health
Avian influenza infections in humans can present a wide spectrum of disease manifestations, ranging from mild to severe. Mild cases often resemble common flu symptoms, including fever, cough, sore throat, and muscle aches. Some individuals may experience conjunctivitis, which is an inflammation of the eye. Symptoms typically appear 3 to 5 days after infection. In more severe cases, avian influenza can lead to serious respiratory complications. Patients may develop pneumonia, acute respiratory distress syndrome (ARDS), and multi-organ failure. These severe manifestations can require hospitalization and intensive medical care (NHS, 2024). The progression to severe disease is influenced by factors such as the specific strain of the virus, the patient’s age, underlying health conditions, and the timeliness of medical intervention. In rare instances, avian influenza infections can result in fatal outcomes. Higher mortality rates are associated with certain highly pathogenic avian influenza (HPAI) strains, such as H5N1 and H7N9. Infected cases may be given antiviral medicine such as oseltamivir or zanamivir, which may help reduce the severity of disease, prevent complications and improve the chances of survival (Smith, 2010).
Human cases of HPAI H5N1 linked to the most recent outbreak in the US
In April 2024, the WHO was notified of a human case of AI H5N1 in Texas. The individual, exposed to infected dairy cattle, developed conjunctivitis. Tests confirmed AI H5N1 clade 2.3.4.4b. The genotype was classified as B3.13, which was the same genotype detected in dairy cattle in Texas. The patient recovered after treatment with oseltamivir and no further cases were linked to this incident. In May 2024, two human cases were reported in Michigan. These unrelated cases were both dairy workers exposed to cattle infected with AI H5N1 clade 2.3.4.4b genotype B3.13. One had conjunctivitis, the other mild respiratory symptoms. Both recovered after treatment with oseltamivir, with no additional cases reported. In July 2024, A fourth case was reported in Colorado, a dairy farm worker exposed to infected cattle. This individual developed conjunctivitis, was treated with oseltamivir, and recovered (UKHSA, 2024).
The CDC have since reported that there are a total of 57 confirmed cases of HPAI H5N1 to date as a result of the most recent US outbreak; 34 cases have been linked to exposure from cattle, 21 from poultry, and 2 from unknown sources (CDC, 2024b).
UKHSA reports of H5N1
A proportion of infections with H5N1 may be asymptomatic. Since 2023, the UK Health Security Agency has received 4 positive human detections of AI H5N1 clade 2.3.4.4b in exposed persons on farms in England where AI H5N1 was also confirmed in the poultry on site. 144 individuals from 8 infected premises have been tested, of which 4 were positive (2.7%). All detections were identified as part of an ongoing enhanced surveillance study of asymptomatic workers exposed to premises infected with AI. It remains unclear whether the detections in these asymptomatic individuals reflected deposition of viral particles on the mucosal surface (in other words, not causing infection) or infection with active viral replication (uncertainty) (UKHSA, 2023).
Global reports of H5N1
Symptomatic human cases of AI H5N1 continue to be detected globally, including cases of clade 2.3.4.4b. Since 2023, prior to the latest human cases in the USA associated with exposure to infected dairy cattle, detections in humans either confirmed to be, or associated with, clade 2.3.4.4b viruses have been reported in Ecuador, China and Chile. These cases were not fatal but did develop severe disease requiring hospitalisation (UKHSA, 2024).
Vulnerable groups
Vulnerable groups vary by strain for influenza. Limited information for B3.13 as is a newly emerging strain. Different groups will be vulnerable to different strains (uncertainty).
Risk characterisation
There is a lack of data concerning the infectious dose of avian influenza A(H5N1) in humans via food consumption. Rare reports exist of potential infection through the consumption of uncooked blood or poultry meat from infected birds, but no detailed studies exist. The lack of presentation of human cases arising from food consumption and the specific circumstances of the reported infections (i.e. from raw duck’s blood) suggests that if infection via food is possible, the infection dose is unlikely be much lower than 107 TCID50 (uncertainty).
Pasteurised cow’s milk and dairy products made from Pasteurised cow’s milk
The available evidence suggests that heat treatment is highly effective at reducing the presence of infectious virus in in milk. Even in a reasonable worst-case scenario (levels as high as 6.3 Log10 EID50/mL of live virus have been detected from bulk milk sampling), effective pasteurisation would be expected to reduce viral titre by >6 Log reduction for Low Temperature Long Time (LTLT) pasteurisation, and between >6 Log reduction and a 4.44 Log reduction in the case of High Temperature Short Time (HTST) pasteurisation. A 4.44 Log reduction, the lowest reduction observed, would result in a maximum post-pasteurisation concentration of live virus of 1.86 Log10 EID50/mL from a starting concentration of 6.3 Log10 EID50/mL. An average serving of milk in the UK as estimated from the National Diet and Nutrition Survey (NDNS) ranges between 70 ml (65+ years) and 150 ml (4-10 years & 11-18 years, NDNS, 2021). Based on these estimates, consumption of 150 ml of contaminated milk that has been pasteurised, would result in a per portion exposure as high as 4.0 Log10 EID50 viral particles. This is approximately 1000 times lower than the hypothesised level needed for infection.
This risk assessment concluded that due to the evidence that pasteurisation is highly effective at reducing the levels of Avian influenza virus under laboratory conditions and the evidence that the oral infectivity of influenza virus in general for humans is extremely low; the probability that UK consumers will receive infectious exposures to influenza of avian origin, on a per portion basis, from the consumption of pasteurised milk, dairy products made with pasteurised milk (e.g., cheese, butter, cream, yoghurt, ice cream) and pasteurised colostrum, if the HPAI strain B3.13 becomes established in the UK dairy herd is assessed to be Negligible. “Negligible” is defined as “So rare that it does not merit to be considered”.
The uncertainty in this assessment is Medium, primarily due to the remaining uncertainty around the effectiveness of pasteurisation in inactivating the virus in milk. There are currently only a few studies that examine the effect of heat treatment on reducing the live virus concentration in milk, with most finding it is highly effective in reducing the levels of infective virus in milk (>6 Log reduction). However, there are at least some reports that which suggests pasteurisation may be less effective at reducing the viral loads. “Medium” uncertainty is defined as “There are some but no complete data available”. If further studies the confirm effectiveness of pasteurisation in inactivating or reducing the virus to negligible levels, then this uncertainty could be reassessed as “low”.
Raw cow’s drinking milk and dairy products made with unpasteurised cow’s milk
UK consumers who drink raw cow drinking milk (RCDM), by contrast, would potentially be exposed to high levels of infective virus. Even allowing for the potential dilution effect of infected milk being mixed in bulk milk tanks with uninfected milk (Bulk milk sampling data found titres in samples positive for infective virus ranging from 1.3 to 6.3 Log10 EID50/mL) UK consumers could still expect to be exposed to significant levels of live virus; a typical portion or serving of milk (150ml glass) could contains much as 8.5 Log10 EID50 infective viral particles per portion of milk consumed, based on an upper concentration level of 6.3 Log10 EID50/mL in the milk.
Due to the potential for high levels of infectious virus to be present in RCDM, the probability that UK consumers would receive infectious exposures to influenza of avian origin, on a per portion basis, from the consumption of RCDM, if the HPAI strain B3.13 becomes established in the UK dairy herd, is assessed to be Medium. “Medium” is defined as “Occurs regularly”. For the assessment of raw colostrum, no specific information was available on the levels of H5N1 strain B3.13 virus present in colostrum from infected cattle but is assumed to be similar to milk, and consequently the per portion risk was also assessed to be Medium.
UK consumers may also be exposed to the virus in the event of an outbreak of H5N1 in UK dairy cattle, if they consume dairy products that were made from the unpasteurised milk from infected cattle. There is currently no extensive data available on the persistence and infectivity of H5N1 strain B3.13 in dairy products made with unpasteurised milk (butter, cream, cheese, yoghurt and ice cream). The production steps for these products can include changes in pH, temperature, salinity and concentration of the dairy substrate that may lead to differential survival and infectivity of the H5N1 virus. Applying a precautionary approach, without data on the survival and infectivity of H5N1 strain B3.13 in the dairy products made from infected milk, it is prudent to assume significant levels of virus may still be present in dairy products made from contaminated unpasteurised milk, consequently the risk was similarly assessed to be the Medium.
The uncertainty in the risk levels above is High, primarily due to the lack of confirmed cases of H5N1 avian influenza, to date, that have been traced back to food consumption, and significant uncertainty around the amount of virus that is required to cause infection from consuming RCDM and dairy products made with unpasteurised milk. Furthermore, comprehensive data regarding whether dairy processes reduce levels or infectivity of the virus is not available. “High Uncertainty” is defined as “There are scarce or no data”.
Severity of infection
In the event of infection, the severity of detriment is assessed to be Low. Recent data from the CDC indicates there have been multiple confirmed human cases of HPAI (H5N1) linked to dairy cattle, with symptoms ranging from milk conjunctivitis to mild respiratory symptoms. As of November 2024, there have been 34 human B3.13 cases associated with cattle (CDC, 2024a), although these may be an underreporting due to mild infections. Most of the human cases were in farm workers; hence, the CDC suggests those who have job-related exposure to dairy cattle, are at a greater risk of contracting HPAI virus (CDC, 2024b). “Low” is defined as "Mild illness: not usually life-threatening, usually no sequelae, normally of short duration, symptoms are self-limiting (e.g., transient diarrhoea). This assumption that the currently circulating strain does not commonly result in severe infection is also informed by the observation that if someone is severely affected by an influenza-like illness in the US they would normally report to medical professionals and be hospitalised and tested. There is therefore some level of confidence that this strain is not resulting in large numbers of severe infections to date.
The uncertainty in this severity is Medium which reflects the recent emergence of this strain, the limited clinical data on infection with this strain so far, and the fact that reporting disincentives make it difficult to be certain that other human infections have not occurred. Additionally, foodborne exposure has not been confirmed and it is unknown whether severity of illness is any different compared to other routes of exposure e.g., inhalation. “Medium” uncertainty is defined as “There are some but no complete data available; evidence is provided in small number of references; authors report conclusions that vary from one another”.
This document specifically assesses the risk from the strain involved in the current outbreak in US dairy cattle (clade 2.3.4.4b genotype B3.13). Strains of influenza vary widely in their clinical presentation in infected humans. However, many human cases of influenza of avian origin have been associated with Asian genotypes or clades. For influenza of avian origin as a whole (in this case, ingested via poultry products), the severity is considered to be High with Medium uncertainty (Kintz et al., 2023).
Key uncertainties
-
More evidence of the efficacy of pasteurisation, particularly HTST, is needed. Contradictory evidence on the effectiveness of pasteurisation has been reported and it is unclear why the variation in results has occurred.
-
There is little data available on the impact of dairy product processing on viral survival and infectivity.
-
Hazard characterisation includes information regarding similar strains due to lack of B3.13 information.
-
Limited information of the volume and manufacturing process of colostrum and colostrum-based products for sale on the UK market.
-
Assumed that dairy products made and sold in the UK will undergo similar methods of production as US products; thus, similar levels of viral infectivity and deactivation may occur. The severity of detriment is assessed as Low based on no evidence of severe illness and no vulnerable groups identified. There has also been no confirmation that severity of illness from foodborne exposure is any different compared to other routes of exposure such as inhalation.
Additional uncertainty: There is very limited information of the volume of RCDM, and dairy products made with unpasteurised milk on the UK market. Whilst this information would not change the per portion risk level determined in this assessment, it is a significant evidence gap that would make it difficult to assess the level of exposure UK consumers face, more generally, in the hypothetical event the H5N1 B3.13 strain were to become prevalent in UK dairy cattle.